
Low testosterone levels have been associated with poor brain function and a higher incidence of dementia in men. A study from the UK Biobank data found that lower total testosterone levels and higher levels of sex-hormone-binding globulin (SHBG) were associated with a higher incidence of dementia (including Alzheimer’s Disease). The men were of an average age of 61 years and were followed for 7 years.
Testosterone is a sex hormone primarily produced in the testes. The adrenal glands also produce a small amount. Testosterone is produced at higher levels in men than in women.
Will taking supplemental testosterone help to improve the symptoms of dementia? How do you know if you have low testosterone? In this post, I will address these questions and more.
What does testosterone do for men?
- Cognition
- Mood regulation
- Helps maintain a sense of wellbeing
- Metabolism. Helps maintain blood glucose levels.
- Deepens a boy’s voice
- Helps with increasing muscle mass.
- Develops and maintains bone.
- Has an impact on body fat distribution.
- Important for the production of sperm.
- Stimulates normal erectile function.
- Involved in the regulation of sex drive.
- Important for the production of red blood cells
- Involved in the production of body hair.
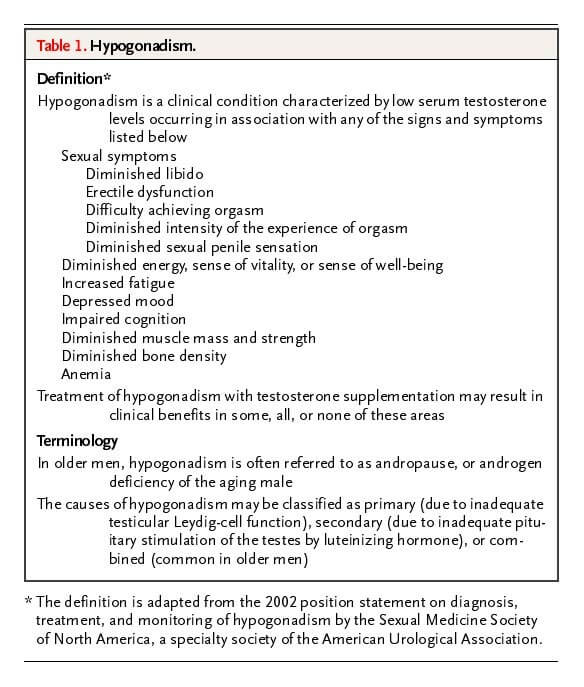
How will you know if you have low testosterone? Male Hypogonadism.
Male hypogonadism (not just low testosterone levels) is diagnosed after taking a detailed history, assessing symptoms and reviewing laboratory tests.
Hypogonadism is a condition that results from the failure of the testis to produce adequate amounts of testosterone. The testes are the gonads. Problems with sperm production may accompany some forms of hypogonadism. Hypogonadism is sometimes described as Low T Syndrome or just Low T.
Hypogonadism may be primary or secondary, and it is further classified into organic or functional. (Table below).
Types of hypogonadism
Table 1.
Classification of Hypogonadism and Causes of Primary and Secondary Hypogonadism
| Primary Hypogonadism | Secondary Hypogonadism |
|---|---|
| ORGANIC | |
| Klinefelter’s Syndrome | Hypothalamic/pituitary tumour |
| Cryptorchidism, myotonic dystrophy, anorchia | Iron overload syndromes |
| Some types of cancer chemotherapy, testicular irradiation/damage, orchidectomy | Infiltrative/destructive disease of the hypothalamus/pituitary |
| Orchitis | Idiopathic hypogonadotropic hypogonadism |
| Testicular trauma, torsion | |
| Advanced age | |
| FUNCTIONAL | |
| Medications (androgen synthesis inhibitors) | Hyperprolactinemia |
| End-stage renal disease * | Opioids, anabolic steroid use, glucocorticoids |
| Alcohol and marijuana abuse * | |
| Systemic illness * | |
| Nutritional deficiency/excessive exercise | |
| Severe obesity, some sleep disorders | |
| Organ failure (liver, heart, and lung) * | |
| Comorbid illness associated with aging * | |
*Combined primary and secondary hypogonadism, but classified to the usual predominant hormonal pattern. Adapted with permission from Bhasin et al.
Symptoms of low testosterone in men
Laboratory tests to diagnose low testosterone
The specific lab tests to diagnose low testosterone levels depend on the suspected underlying condition, but the ones commonly used in Functional Medicine are the ones listed below:
- Total and free testosterone (Or free androgen index)
- Sex Hormone Binding Globulin (SHBG)
- Blood glucose (Fasting and post-meal or CGM)
- Zinc levels
- Iron studies
- FSH, LH, Prolactin
Do testosterone levels decline with age?
Unlike women and menopause, men do not have well-defined criteria that define “male menopause or andropause”. Men can produce sperm their whole life, and testosterone levels do not reflect age. Many younger men have alarmingly low testosterone levels. Studies have shown declining levels of testosterone in young adult men (Lokeshwar et al 2021.
What levels of total testosterone are considered normal?
This is a simple question with a complex answer. Instead of a single normal level for total testosterone, normal men have a wide range. Testosterone levels between 270 and 1,070 nanograms per deciliter (ng/dL) (9.369 nmol/L to 37.129 nmol/L) are considered normal.
Testosterone levels decline after the age of 40, perhaps even earlier now.
The paper’s title in The Journal Of Urology states this well: “What Is a Normal Testosterone Level for Young Men? Rethinking the 300 ng/dL Cutoff for Testosterone Deficiency in Men 20-44 Years Old.
| Age in years | Total Testosterone Levels (ng/dL) |
|---|---|
| 20-24 | 409-558 |
| 25-29 | 413-575 |
| 30-34 | 359-498 |
| 35-39 | 352-478 |
| 40-44 | 350-473 |
Does taking supplemental testosterone improve cognition?
If low testosterone levels are associated with higher risks of dementia, logically it would follow that adding supplemental testosterone should reduce those risks. This is where we need interventional studies. Association studies are large population-based studies but cannot tell us about causation. This means that large studies like the UK Biobank study I referred to earlier, cannot tell whether those men had dementia because of the low testosterone and high SHBG or if there were other factors.
Interventional studies are those where one group of people of similar age and metrics are given the intervention (testosterone, in this case), and another group is given a placebo. Both groups are followed for some time (the duration depends on the length of the study) to see if there are any significant differences in both groups. Basically, did the men given testosterone do better in terms of brain health than those who were not?
Biology is complex!
Some studies of testosterone replacement found benefits in cognition, but others did not.
A systemic review and meta-analysis (a study of studies) by Buskbjerg et al,2019 concluded: “…the available RCTs (randomized controlled trials) do not support a beneficial effect of TS (testosterone replacement) on cognitive functioning in men with testosterone levels within normal ranges. There is, thus, no evidence for prescribing TS for improving cognitive functioning in men with no clinical signs of hypogonadism,” The most important question is why were men with normal testosterone levels prescribed testosterone?
Other studies ( Wahjoepramono et al 2016) found modest cognitive benefits of using testosterone in older men.
Several factors may explain this discrepancy.
- Age. We know that dementias like Alzheimer’s Disease develop 20-30 years before someone has symptoms. We also know that mid-life poor health (high blood pressure, high triglycerides, metabolic syndrome) are risk factors for dementia. Is it possible that raising testosterone levels (not necessarily by using testosterone replacement) earlier in life rather than later will show benefits? We have to wait for the studies.
- Using testosterone in men with memory symptoms: Is it too little too late? There is a window of opportunity regarding benefits in women and hormone therapy. Starting hormone therapy soon after menopause (5-6 years) shows better benefits versus starting later. We do not know whether there is a similar window of opportunity in men.
- Estrogen levels in men. Men make estrogen too! In fact, men make more estrogen than women in menopause. Many of the brain benefits of testosterone in men may come from its conversion to estrogen (Russel, 2019). The brain can make testosterone and estrogens locally. However, blood levels of estrogen may not reflect levels in the brain.
- Sex Hormone Binding Globulin (SHBG). Sex hormones circulate in the blood bound to proteins like SHBG. The levels of free hormones have the largest impact on hormone function. Hormones bound to SHBG are not free to act on tissues. A paper in the journal Andrology, 2020, showed that pre-treatment levels of SHBG decide the effects of testosterone replacement. In fact, SHBG is an independent risk factor for heart disease, stroke and dementia.
- Type and dosage of testosterone replacement. Testosterone is given as gel, cream injections or orally (harmful). Each type has a different action on the body. Therefore comparing studies using gels or creams with injections is like comparing apples with oranges. Monitoring testosterone levels in the blood when using gels or cream may not be accurate.
- Type 2 Diabetes and testosterone. We know that having type 2 diabetes dramatically raises your risk for dementia. Additionally, men with diabetes are at a very high risk of hypogonadism. A study reported that over 11 years of using injectable testosterone, men with diabetes went into remission, which means they were not considered to have diabetes anymore. However, these men were on diabetes medication initially.
- Lifestyle modifications along with testosterone replacement. We have plenty of data supporting the prevention of dementia through a healthy lifestyle. Single causes do not cause dementia. Using a multimodal approach of lifestyle AND testosterone may show more cognitive benefits. In fact, the LITROS study (Lifestyle Intervention and Testosterone Replacement in Obese Seniors) showed that.
- Appropriate brain tests. An important question is how cognition was assessed in the study participants. Did they use brain imaging versus simple questionnaires? Simple questionnaires cannot detect subtle changes.
Should you get a cognitive assessment done?
Does supplemental testosterone benefit other health conditions?
Testosterone therapy in hypogonadal men has shown benefits in the following areas: (Morgantaler et al 2022, Haider et al 2020)
- Libido and erections
- Physical activity
- Sense of increased energy
- Better mood
- Improved bone density and bone strength
- Resolution of unexplained anemia
- Remission of type 2 diabetes
What does this mean for you?
There are no simple answers! You need to discuss with a knowledgeable clinician to understand what applies to you.
Using testosterone replacement is not for you if you are looking at fertility. Testosterone will make you infertile. Other ways to increase testosterone levels include prioritizing protein intake, improving sleep, exercise, supplements like omega 3 fatty acids, and correcting zinc and vitamin D3 deficiencies.
Medications like clomiphene and HCG can raise testosterone levels.
Action steps:
- Fill out the qADAM questionnaire to check your symptom severity.
2) Get appropriate lab tests done.
3) Meet a knowledgeable doctor with your questionnaire and lab reports to discuss what applies to you.
References
- Marriott, Ross J., et al. “Lower serum testosterone concentrations are associated with a higher incidence of dementia in men: The UK Biobank prospective cohort study.” Alzheimer’s & Dementia (2022).
- Lokeshwar, Soum D., et al. “Decline in serum testosterone levels among adolescent and young adult men in the USA.” European urology focus 7.4 (2021): 886-889.
- Zhu, Alex, et al. “What is a normal testosterone level for young men? Rethinking the 300 ng/dL cutoff for testosterone deficiency in men 20-44 years old.” The Journal of Urology 208.6 (2022): 1295-1302.
- Zitzmann, Michael. “Testosterone and the brain.” The Aging Male 9.4 (2006): 195-199.
- Buskbjerg, Cecilie R., et al. “Testosterone supplementation and cognitive functioning in men—a systematic review and meta-analysis.” Journal of the Endocrine Society 3.8 (2019): 1465-1484.
- J Wahjoepramono, Eka, et al. “The effects of testosterone supplementation on cognitive functioning in older men.” CNS & Neurological Disorders-Drug Targets (Formerly Current Drug Targets-CNS & Neurological Disorders) 15.3 (2016): 337-343.
- Russell, Nicholas, and Mathis Grossmann. “Mechanisms in endocrinology: estradiol as a male hormone.” European Journal of Endocrinology 181.1 (2019): R23-R43.
- Ramachandran, Sudarshan, Geoffrey I. Hackett, and Richard C. Strange. “Testosterone replacement therapy: Pre‐treatment sex hormone‐binding globulin levels and age may identify clinical subgroups.” Andrology 8.5 (2020): 1222-1232.
- Rhoden, Ernani Luis, and Abraham Morgentaler. “Risks of testosterone-replacement therapy and recommendations for monitoring.” New England Journal of Medicine 350.5 (2004): 482-492.
- Hassen, Céline Ben, et al. “Association between age at onset of multimorbidity and incidence of dementia: 30-year follow-up in Whitehall II prospective cohort study.” bmj 376 (2022).
- Morgentaler, Abraham, et al. “Recognizing the True Value of Testosterone Therapy in Health Care.” Androgens: Clinical Research and Therapeutics 3.1 (2022): 217-223.
- Haider, Karim Sultan, et al. “Remission of type 2 diabetes following long‐term treatment with injectable testosterone undecanoate in patients with hypogonadism and type 2 diabetes: 11‐year data from a real‐world registry study.” Diabetes, Obesity and Metabolism 22.11 (2020): 2055-2068.
- Gregori, Giulia, et al. “Cognitive response to testosterone replacement added to intensive lifestyle intervention in older men with obesity and hypogonadism: prespecified secondary analyses of a randomized clinical trial.” The American Journal of Clinical Nutrition 114.5 (2021): 1590-1599.

