(Updated from an earlier version on the MDS Program website)
Often we hear that Intermittent Fasting/Time-Restricted Eating (TRE/IF) is just a different version of a low-calorie diet. Is that true? While it is true that when you follow a TRE/IF way of eating, you do end up eating less food than you would otherwise do, the critical difference is on TRE/IF you don’t have to deliberately, consciously monitor the amount of food you eat; it happens by default! You feel less hungry! (For convenience, I will consider a fasting period of 24 hours or longer as Intermittent Fasting, while a fasting window of fewer than 24 hours is Time-Restricted Eating)
On a low-calorie diet, you get what I call the “Revenge of the Deprived Calorie.” Hunger is worse, which is one of the reasons why this diet is not sustainable long-term. ((Ref)) Additionally, on a low-calorie diet, your metabolic rate reduces. Reducing your metabolic rate is not good for weight loss. ((Ref))
Are there any other factors that differentiate a low-calorie diet from TRE/IF?
COMPARISON OF LOW-CALORIE DIETS WITH INTERMITTENT FASTING
| FEATURES | LOW-CALORIE DIET | INTERMITTENT FASTING |
| Weight Loss | Yes, but not sustained over long-term | Yes. Long-term studies have not been done, but case reports show long-term benefits are maintained. |
| Fat-Free Mass (FFM) | Reduced | Less reduction compared to a low-calorie diet. |
| Hunger | Often not reduced. This is why compliance is difficult | Hunger reduced. |
| Muscle Loss | May be expected | Usually, no muscle loss |
| Ease of following the plan | Difficult for some | Most people find this easy to adapt to their lives. |
| Brain Function | Usually unchanged | Most people report better brain function. Less “brain fog.” |
| Metabolic Rate | Usually reduced | Metabolic rate increased |
| Fasting Insulin | Reduced | Higher reduction than in calorie-restricted diet |
| Growth Hormone (GH) (Preserves muscle mass) | No change in GH | Increased secretion of GH |
Weight Loss
In studies comparing a calorie-restricted diet with intermittent fasting, both are equally effective for weight loss. In clinical studies, these are called Daily Calorie Restriction (DCR) versus Intermittent Calorie Restriction (ICR). However, the type of weight loss was different in the two methods. ((Ref))
Change In Body Composition
Although total weight loss is the focus of most weight loss programs, the change in body composition significantly impacts long-term results. What do I mean by that?
Your body weight includes fat, muscles, bone, organs and body fluids. You are interested in fat loss, and you don’t want to lose bone and not your muscles! Fat-free mass (FFM) is the part of your weight that includes everything OTHER than your body fat.
Fat-free mass (FFM) is extremely important for long-term weight loss. FFM decides your metabolic rate. The higher the amount of FFM, the higher is your metabolic rate. Therefore, you don’t want to lose FFM.
In most studies, weight loss by Daily Caloric Restriction resulted in a 75–80% decrease in fat mass and a 20–25% decrease in FFM. However, Intermittent Caloric Restriction showed a 90% weight loss of fat and 10% weight loss of FFM. ((Ref))
In a study on postmenopausal women ((Ref)), the authors looked at comparing the long-term (1 year) effects of moderate versus severe energy restriction on body composition. Those in the moderate energy restriction group reduced their energy intake by 25-35%. The severe energy restriction group reduced their energy intake by 65-75% for four months, followed by eight months of moderate energy restriction.
What did they find?
The amount of weight lost by those on the severe energy-restricted diet was about two times more than those on moderate calorie restriction. The loss in muscles was also proportional to the weight loss. This means that people who lost more weight also lost more muscle mass (FFM).
Bone Loss:
A somewhat disconcerting effect was seen on Bone Mineral Density (BMD). Those women on the moderate energy-restricted diet lost about as much bone density as similar-aged postmenopausal women. Still, those on the severe energy-restricted diet didn’t fare as well.
In the severe energy-restricted group, the bone loss continued over a whole year! These women were asked to eat proteins at 1 gram/kilogram of body weight, and the meal replacement product they used contained adequate vitamin D and calcium. (Bone density is affected by protein intake, vitamin D3 and calcium). The women were not on hormone therapy.
Hunger
One of the most prominent weight loss problems by using a low calorie or calorie-restricted diet is hunger, and weight regain. The increase in hunger (The Revenge of The Deprived Calorie) is compounded by a reduction in metabolic rate.
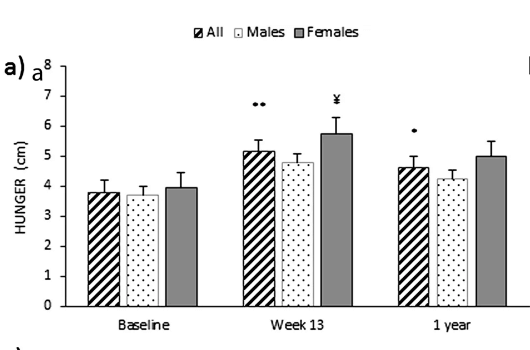
In a study reported in the International Journal Of Obesity, the authors looked at hunger and feelings of fullness in a group of men and women who had successfully lost weight on a very low-calorie diet. At the end of 1 year, they maintained a 15% weight loss, but hunger had increased, though post-meal fullness had increased as well. Women felt hungrier than men! As you can see in the image Fig 1, at 13 weeks, hunger was higher than at the end of 1 year. Interestingly, hunger levels were higher after weight loss than at baseline. ((Ref))
Alternate-day fasting and hunger: In a study of alternate-day fasting for weight loss, there was no increase in hunger at the end of 8 weeks of the study period. ((Ref))
Many factors control hunger. However, eating more protein and fewer carbohydrates keeps you satiated longer.
Number of Calories Consumed
Reducing daily calorie intake below the baseline is one of the most typical methods used for weight loss. The calorie restriction varies, and most calorie-restricted diets aim to reduce daily calories by at least 15-40% of the baseline energy requirement.
In studies on alternate-day “fasting,” where participants were allowed to eat 25 % of their calculated calorie requirement on ‘fast” days and 100 % on non-fast days, they found that people ate 20–30% of their energy needs on “fast “days, while on the eating days, they ate 100–110% of energy needs. Therefore, were they eating more or did it even out over several days?
When they calculated energy restriction over 48 hours (fast+eat days), they found that most people achieved 35-38% energy restriction. This was despite eating more on “eat” days and not consciously counting calories. However, those on daily calorie restriction managed only 18-23% energy restriction daily.
Metabolic Rate
Many of you ask me, “How can I increase my metabolism?” What does this mean?
Basal Metabolic Rate (BMR) is the number of calories your body needs to maintain essential body functions like breathing, circulation, digestion, and temperature regulation. BMR is used interchangeably with the term Resting Energy Expenditure (REE). REE includes BMR plus the energy used in sitting, moving around etc. REE has a massive impact on long-term weight loss.
In the MATADOR study, men with obesity were divided into two arms, one arm on continuous energy restriction and the other on intermittent energy restriction. Weight loss reduces REE. However, in this study, they found that people on intermittent energy restriction had a minor reduction of REE compared to those on continuous calorie restriction ((Ref))
I have mentioned the “Biggest Loser “Study before. They followed a low-calorie diet. After six years, they were found to have a lower metabolic rate. ((Ref))
Insulin Levels
Fasting insulin levels are an important factor in weight loss. As this paper reports, they observed that higher fasting insulin levels were related to a higher weight over ten years. ((Ref)). Therefore, the eating plan that works best at lowering insulin levels should work better for fat loss.
Food and Insulin:
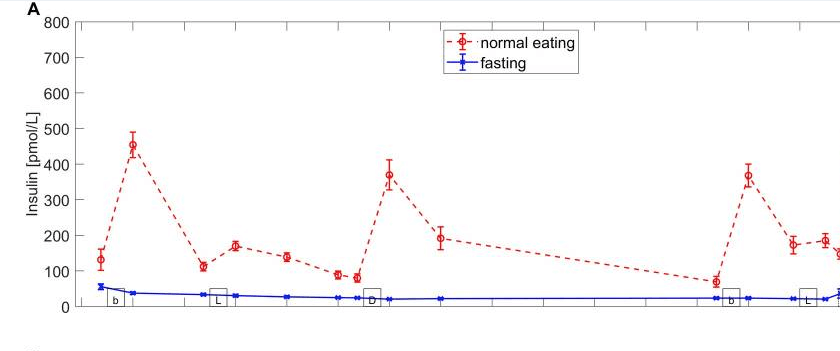
When you eat food, your insulin levels rise. Eating carbohydrates spike your insulin and blood glucose levels the most, followed by proteins and fat. As you can see in the image below (Fig.2), the graph in red shows the levels of insulin throughout the day in a person who is eating three meals and two snacks a day. The higher red peaks are the major meals, and the smaller ones are snacks.
The blue graph represents insulin levels while fasting. As you can see, the “area under the curve” (AUC) with normal eating is much bigger than the area under the fasting curve.
Your insulin levels do not increase when you don’t eat, i.e., when you fast, your insulin levels fall.
Growth Hormone (GH)
From the perspective of retaining muscle mass, Growth Hormone levels are critical. Adults with GH deficiency have more belly fat, worse lipid profiles and increased heart disease risks. ((Ref))
In a 5- day fasting study, levels of GH were higher than in people who were not fasting. In fact, on day 1 of the fast, GH levels were about three times higher than baseline! ((Ref))
Bottomline
- Continuous calorie restriction and intermittent calorie restriction (TRE/IF) both lead to weight loss.
- TRE/IF is easier to implement and stick to.
- Hunger is less on TRE/IF and therefore it is easier to use long-term.
- Severe energy restriction (aka low-calorie diet) leads to higher weight loss, but at the cost of higher bone loss.
- Insulin levels reduce more on TRE/IF than on a low-calorie diet.
- Growth Hormone levels increase with fasting. This helps in maintaining a leaner body.
- Fat-free Mass is preserved on TRE/IF versus on continuous calorie restriction (low-calorie diet).


